Statin-Antifungal Interaction Checker
Check if your statin and antifungal combination is safe. This tool identifies dangerous interactions and recommends safer alternatives based on medical evidence.
When you're taking a statin to lower your cholesterol, and your doctor prescribes an antifungal for a stubborn infection, you might not think twice. But behind the scenes, these two medications can collide in your body in ways that are dangerous - even life-threatening. The problem isn't rare. It happens often, and most people don't know about it until it's too late.
Why This Interaction Isn't Just a Warning on a Label
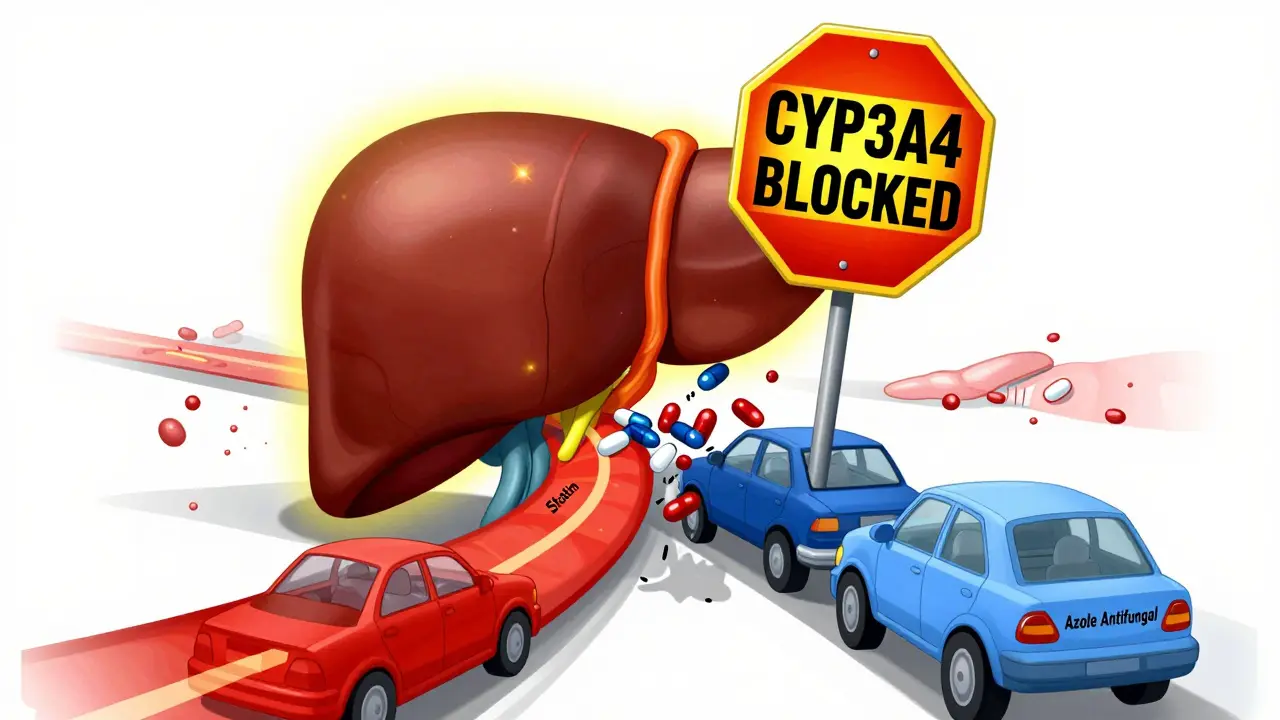
Systemic antifungals - especially the azole class like fluconazole, itraconazole, and posaconazole - don't just fight fungi. They also shut down key enzymes in your liver that break down other drugs. One of those enzymes, CYP3A4, is responsible for clearing more than 30% of all prescription medications from your bloodstream. When azoles block it, statins build up like traffic on a highway with no exits. Statins like simvastatin, lovastatin, and atorvastatin rely heavily on CYP3A4 to get processed. When you take them with a strong inhibitor like posaconazole, your statin levels can spike 10 to 20 times higher than normal. That doesn’t just mean you’ll feel sore. It means your muscles can start breaking down - a condition called rhabdomyolysis. In severe cases, this leads to kidney failure, hospitalization, or death.Not All Statins Are Created Equal
If you're on a statin and need an antifungal, not all options are equally risky. The big three - simvastatin, lovastatin, and atorvastatin - are the most dangerous when paired with azoles. They’re like gasoline near an open flame. On the other hand, pravastatin and rosuvastatin are much safer. Why? Because they don’t depend on CYP3A4. Pravastatin is cleared mostly by the kidneys, and rosuvastatin uses a mix of pathways. That’s why experts say: if you need an antifungal, switch to one of these two - at a lower dose. But even that’s not foolproof. Ketoconazole, a powerful antifungal, can still raise pravastatin and rosuvastatin levels by blocking a different transporter called OATP1B1. So even the "safer" statins aren’t risk-free. The key is knowing which antifungal you’re getting and how it behaves.Immunosuppressants Make It Worse
If you’ve had a transplant, you’re already on a drug like cyclosporine or tacrolimus. These help your body accept the new organ - but they also block CYP3A4 and P-glycoprotein, the same systems statins need to leave your body. The result? A double whammy. Studies show that when transplant patients take statins with cyclosporine, their statin levels can jump 3 to 20 times higher than normal. One study found that up to 25% of these patients developed muscle pain or damage. In extreme cases, creatine kinase (CK) levels - a marker of muscle breakdown - soared past 10,000 U/L. Normal is under 200 U/L. This isn’t theoretical. Emergency rooms see these cases. A 62-year-old man on simvastatin and cyclosporine after a kidney transplant developed severe muscle weakness, dark urine, and kidney failure. His CK hit 28,000 U/L. He survived, but barely. This happens more often than you think.
Which Antifungals Are the Worst?
Not all azoles are the same. Here’s how they stack up:- Ketoconazole: Strongest CYP3A4 inhibitor. Banned in many countries for systemic use because of liver damage and interactions. Never combine with any statin.
- Posaconazole: Also a strong inhibitor. Long half-life (24-30 hours), meaning it sticks around even after you stop taking it. Statins must be paused during and for several days after treatment.
- Itraconazole: Potent CYP3A4 blocker. Increases simvastatin levels by 15-20 times. Avoid completely.
- Voriconazole: Moderate to strong inhibitor. Use with caution. Monitor closely.
- Fluconazole: Weakest of the azoles. Only moderate CYP3A4 inhibition. Still risky with high-dose statins, but safer than the others.
If you’re prescribed an antifungal, ask: "Which one is it?" If it’s ketoconazole or itraconazole, you should not be on any CYP3A4-metabolized statin. Period.
What Should You Do? A Clear Action Plan
If you’re on a statin and need an antifungal, here’s what actually works:- Stop the risky statin. If you’re on simvastatin, lovastatin, or atorvastatin, pause it entirely during antifungal treatment. Don’t wait for symptoms.
- Switch to pravastatin or rosuvastatin. Use the lowest effective dose - 10 mg daily for pravastatin, 5-10 mg for rosuvastatin.
- Check your kidney function. Both antifungals and statins can strain your kidneys. Get a basic blood test before starting.
- Watch for muscle pain. If you feel unexplained soreness, weakness, or dark urine, stop the statin and call your doctor immediately.
- Wait before restarting. After finishing an antifungal like posaconazole, wait at least 3-5 days before restarting your statin. Its effects linger.
For transplant patients: Your care team should be monitoring your immunosuppressant levels closely. When an azole is added, they should reduce your cyclosporine or tacrolimus dose by 30-50% to avoid toxicity. This isn’t optional - it’s standard.
Why This Keeps Happening
You’d think doctors would know better. But here’s the ugly truth: these dangerous combinations are still prescribed regularly. A 2012 study found that despite clear warnings on drug labels, doctors kept prescribing simvastatin with azoles. Why? Time pressure. Overworked clinics. Lack of alerts. Many electronic health systems still don’t flag these interactions unless they’re flagged by pharmacists. The good news? Hospitals that use pharmacist-led reviews have cut these dangerous prescriptions by over 60%. At Melbourne’s Royal Melbourne Hospital, a simple protocol requiring pharmacist sign-off before dispensing azoles reduced risky statin-azole combos by 63%. That’s not luck - that’s system change.What’s Changing Now?
The future isn’t all bad. Newer antifungals like isavuconazole and olorofim are being developed with fewer drug interactions. Olorofim, in particular, doesn’t touch CYP3A4 at all - a game-changer for patients on statins. Also, genetic testing is starting to help. About 12% of people have a gene variation (SLCO1B1) that makes them extra sensitive to statin side effects. If you’ve had muscle pain on statins before, ask about this test. It could save you from a future crisis.Bottom Line: Don’t Guess. Ask.
You don’t need to memorize enzyme pathways. But you do need to ask three simple questions:- "Is this antifungal going to interact with my statin?"
- "Can I switch to pravastatin or rosuvastatin while I’m on it?"
- "What should I do if I feel muscle pain?"
If your doctor says "It’s fine," ask for the evidence. If they don’t know, insist on a pharmacist consult. These interactions aren’t rare mistakes - they’re preventable tragedies.
Statins save lives. Antifungals save lives. But when they meet without caution, they can destroy muscle, kidneys, and even your future. Knowledge isn’t power here - it’s protection.















Comments (12)